I do think it would be a good idea to ask the medical advisors for this forum to respond to this paper.
We must remember this is a cadaver study and the question cannot be answered if a nerve was or was not gliding freely. It might be an assumption one might conclude but cannot be proofed.
I do not know how many of the physicians who do pudendal decompression surgery monitor the activity of the pudendal nerve during surgery. I know some of them do. If the activity of the nerve improves during surgery then that is a functional assessment of what is happening to the nerve and to me the functional activity of the nerve is the most important indicator of improvement in the nerve to conduct electrical impulses. Cadaver studies cannot answer questions about the effect of the tissue surrounding the pudendal nerve on its functional activity.
As I wrote in an early post not all connective tissue is created equal and the authors did not analyze the type of connective tissue to show that it is "scar tissue."
I do think this paper raises an important question about entrapment of the pudendal nerve and that entrapment may or may not be the "gold" standard to use to determine if a patient is a candidate for surgery. However, this would be true for any nerve in the body such as carpal tunnel.
Publication Abstract - A Must Read!
Re: Publication Abstract - A Must Read!
2/07 LAVH and TOT 7/07 TOT right side removed 9/07 IL, IH and GN neuropathy 11/07 PN - Dr. Howard
6/08 Obturator neuralgia - Dr. Conway 11/08 Disability, piriformis syndrome - Dr. Howard
4/09 Bilateral obturator decompression surgery, BLL RSD - Dr. Howard
9/10 Removed left side TOT, botox, re-evaluate obturator nerve - Dr. Hibner
2/11 LFCN and saphenous neuralgia - Dr. Dellon 2/11 MRI with Dr. Potter - confirmed entrapment
5/11 Right side TG - Dr. Hibner 2012 Left side TG - Dr. Hibner
6/08 Obturator neuralgia - Dr. Conway 11/08 Disability, piriformis syndrome - Dr. Howard
4/09 Bilateral obturator decompression surgery, BLL RSD - Dr. Howard
9/10 Removed left side TOT, botox, re-evaluate obturator nerve - Dr. Hibner
2/11 LFCN and saphenous neuralgia - Dr. Dellon 2/11 MRI with Dr. Potter - confirmed entrapment
5/11 Right side TG - Dr. Hibner 2012 Left side TG - Dr. Hibner
Re: Publication Abstract - A Must Read!
This will be my last visit here. This perhaps isn't the proper place to make this post but I would like to comment on the above referenced study and believe my experience will give valuable input to those who question the validity of the pne diagnosis. I do not have pn. I do not have pne. I have a set of symptoms that would lead one to believe that my pudendal nerve is irritated or entrapped. This is not the case (actually, it may very well be entrapped but it doesn't matter). I have referred pain from the location in my spine from which the sympathetic fibers of the pudendal nerve originate. As I have stated before, the mechanism behind this referral is similar to a person who has a heart attack and gets pain in their arm. The sympathetic nerves from the heart are firing and the brain cannot differentiate between the nerves from the heart and the nerves to the arm. In my case their is a compression of the nerves in the thoracolumbar junction and my brain is interpreting that as pain from the pudendal nerve. It is a relatively simple theory. My pain is rapidly receding. I am back to work in a light duty capacity and sit all day long if I want to. I lift weights. I do squats. I no longer fear the dreaded pne diagnosis. It is my opinion that outside of a direct surgical insult to the pudendal nerve, pne does not exist.
People, like myself, often come to this forum out of fear. Fear of a diagnosis that is incurable. These people need reassurance. They need to calm down. They need to know that they can live a good life. A life that involves sitting, weightlifting and whatever else they may like to do. They do not need to be told to lower their expectations or that if they are lucky they may be able to work again. They do not need the idea of surgery crammed down there throats. New ideas should be encouraged and success stories should be taken seriously. People who advocate for successful treatments that do not involve surgery should be celebrated; not banned from the forum. What exactly are we trying to accomplish here? Is it more important to be right or for people to get better?
I thank God for ezer and his mind body ideas everyday. He helped me to break the cycle of fear and pain. Without him I would never have been still long enough for God to lead me to the cause of my pain. I still use many of the tools he has given me. I understand that he is a strong personality and is at times condescending (sorry ezer). But don't we need people to stand firmly against a surgery that is hurting more people than it is helping? Don't we need more success stories? This is a serious topic and needs to be treated as such. People come to this forum and read stories about a nerve block permanently making people worse or bending over causing years of pain. This is insane! we are not made of glass! My God did not create me to fear sitting down or to become permanently bed ridden because I picked up my child. Pain is complex. Lets stop ignoring the science that discounts a simple cause and effect approach to pain. I have learned a great deal on this forum. Mostly about what I shouldn't do.
Violet, I appreciate the time you take out of your life to run this forum. I know your heart is for helping people. The world could use more people like you.
Seth
People, like myself, often come to this forum out of fear. Fear of a diagnosis that is incurable. These people need reassurance. They need to calm down. They need to know that they can live a good life. A life that involves sitting, weightlifting and whatever else they may like to do. They do not need to be told to lower their expectations or that if they are lucky they may be able to work again. They do not need the idea of surgery crammed down there throats. New ideas should be encouraged and success stories should be taken seriously. People who advocate for successful treatments that do not involve surgery should be celebrated; not banned from the forum. What exactly are we trying to accomplish here? Is it more important to be right or for people to get better?
I thank God for ezer and his mind body ideas everyday. He helped me to break the cycle of fear and pain. Without him I would never have been still long enough for God to lead me to the cause of my pain. I still use many of the tools he has given me. I understand that he is a strong personality and is at times condescending (sorry ezer). But don't we need people to stand firmly against a surgery that is hurting more people than it is helping? Don't we need more success stories? This is a serious topic and needs to be treated as such. People come to this forum and read stories about a nerve block permanently making people worse or bending over causing years of pain. This is insane! we are not made of glass! My God did not create me to fear sitting down or to become permanently bed ridden because I picked up my child. Pain is complex. Lets stop ignoring the science that discounts a simple cause and effect approach to pain. I have learned a great deal on this forum. Mostly about what I shouldn't do.
Violet, I appreciate the time you take out of your life to run this forum. I know your heart is for helping people. The world could use more people like you.
Seth
-
stephanies
- Posts: 692
- Joined: Mon Oct 25, 2010 3:07 am
Re: Publication Abstract - A Must Read!
I am not much for debate and back-and-forth, nor do I have a medical background, but I will say that the forum part of this web-site that is used to ask questions and exchange ideas is, in my opinion,very valuable. I don't see that it is cramming surgery down anyone's throats, I feel the discussion of treatment modalities other than surgery is quite robust. Do I think the PN doctors have some work to do in providing/publishing data and answering questions? Absolutely. Do I think the old PN protocol (PT, 3 nerve blocks, Botox) needs revision? Absolutely. Do I believe every PN doctor or PT I have seen has been honest and straight forward with me? No. I also believe that we don't all have to agree on why our pain exists or find the same treatments for the pain. We are all different and may have similar pain caused by vastly different things. The forum should be a place of learning and compassion. I think if at any time, anyone feels like the forum is leading him/her in a dark, unhealthy direction, it is probably time to take a break or move on.
Stephanies
Stephanies
PN started 2004 from fall. Surgery with Filler Nov. 2006, Dr. Campbell April 2007. Pain decreased by 85% in 2008 (rectal and sitting pain resolved completely), pain returned in 12/13. Pain reduced significantly beginning around 11/23.
-
cpps-admin
- Posts: 41
- Joined: Tue Aug 05, 2014 8:29 am
Re: Publication Abstract - A Must Read!
For me, one of the most interesting things about this study, other than the fact that all pudendal nerves are attached by connective tissue to multiple sites, is the complexity of the region in which the PNE surgeons operate. It's a minefield  I would not want any old surgeon messing about there, truly. This is not a simple operation; don't ever let anyone tell you that it is. Moreover, the cadavers show the wide variability of the nerve and its multiple trunks and diverse branching patterns. We all have pudendal nerves that are slightly differently located and which branch in different places, making any operation on this nerve fraught with difficulty. The nerve is only about 4.5mm wide, hidden away in a mass of muscle, sinew and connective tissue.
I would not want any old surgeon messing about there, truly. This is not a simple operation; don't ever let anyone tell you that it is. Moreover, the cadavers show the wide variability of the nerve and its multiple trunks and diverse branching patterns. We all have pudendal nerves that are slightly differently located and which branch in different places, making any operation on this nerve fraught with difficulty. The nerve is only about 4.5mm wide, hidden away in a mass of muscle, sinew and connective tissue.
The study ends with these wise words of warning:
The study ends with these wise words of warning:
As health care providers, we should carefully weigh the risks and benefits of interventional procedures with limited clinical efficacy and potential for significant complications. A comprehensive knowledge of the complex pudendal nerve anatomy is essential in optimizing diagnostic and treatment modalities.
I am the admin of the member forum at a chronic prostatitis (aka CPPS) website
Re: Publication Abstract - A Must Read!
cpps-admin, there have been multiple studies over more than a decade demonstrating the variations in the branching of the pudendal nerve for example some individuals the rectal branch branches before Alcock's canal, in some individuals after Alcock's canal and in a small subset it is a totally separate branch from the main branch of the pudendal coming off of S2 alone. Therefore, the variations in the branching of the pudendal nerve is not new. There are variations in the branches and even slight deviations of the paths of nerves of all the anatomical nerve publications I've ever read for example genitofemoral nerve. However, it does speak to the importance that physicians know the variations they may encounter during surgery. The technology is not to the level yet that these variations can be seen on an MRI prior to surgery so that a physician would know before they opened you what exactly the anatomy of your pudendal nerve was. I anticipate as the resolution of MRI advances this technology in years to come will be available.
All surgeries carry risk. I am not a surgeon I cannot make a statement whether this surgery is a simple one or not. For a neurosurgeon like Ben Carson, this might be a walk in the park compared to separating conjoined twins. P.S. I am not going down the political debate here, just thought he was a good example so let's not get off topic with him .
.
All surgeries carry risk. I am not a surgeon I cannot make a statement whether this surgery is a simple one or not. For a neurosurgeon like Ben Carson, this might be a walk in the park compared to separating conjoined twins. P.S. I am not going down the political debate here, just thought he was a good example so let's not get off topic with him
2/07 LAVH and TOT 7/07 TOT right side removed 9/07 IL, IH and GN neuropathy 11/07 PN - Dr. Howard
6/08 Obturator neuralgia - Dr. Conway 11/08 Disability, piriformis syndrome - Dr. Howard
4/09 Bilateral obturator decompression surgery, BLL RSD - Dr. Howard
9/10 Removed left side TOT, botox, re-evaluate obturator nerve - Dr. Hibner
2/11 LFCN and saphenous neuralgia - Dr. Dellon 2/11 MRI with Dr. Potter - confirmed entrapment
5/11 Right side TG - Dr. Hibner 2012 Left side TG - Dr. Hibner
6/08 Obturator neuralgia - Dr. Conway 11/08 Disability, piriformis syndrome - Dr. Howard
4/09 Bilateral obturator decompression surgery, BLL RSD - Dr. Howard
9/10 Removed left side TOT, botox, re-evaluate obturator nerve - Dr. Hibner
2/11 LFCN and saphenous neuralgia - Dr. Dellon 2/11 MRI with Dr. Potter - confirmed entrapment
5/11 Right side TG - Dr. Hibner 2012 Left side TG - Dr. Hibner
-
cpps-admin
- Posts: 41
- Joined: Tue Aug 05, 2014 8:29 am
Re: Publication Abstract - A Must Read!
I think what I was trying to say is that because the nerve locations can be so diverse, every surgery is complex, no matter how skilled the surgeon. Each new PN operation is like walking through a minefield, because to get to where you want to go, you have to pick carefully through a jungle of unpredictably located nerves and blood vessels. The surgeon has to be alert, very alert, on the ball at all times. Nothing here is routine. No time for chit chat with the surgical assistants. If you've attended operations, as I have, you'll know the sort of banter that goes on in operating rooms. This operation wouldn't allow for much of that, if any.nyt wrote:the variations in the branching of the pudendal nerve is not new. ... However, it does speak to the importance that physicians know the variations they may encounter during surgery.
Yes, but some more than others. This paper clearly implies that this surgery is of the more risky variety.All surgeries carry risk.
Indeed, which is why we should rely on the opinion of the authors of the paper. They are surgeons, and they state that this surgery is complex. This paper comes from a very respected center, so I'll take the opinions expressed at face value.I am not a surgeon I cannot make a statement whether this surgery is a simple one or not.
I am the admin of the member forum at a chronic prostatitis (aka CPPS) website
-
stephanies
- Posts: 692
- Joined: Mon Oct 25, 2010 3:07 am
Re: Publication Abstract - A Must Read!
A close family member of mine had neurosurgery with Dr. Carson when he was a very small infant. When Dr. Carson was asked about the difficulty of the procedure, as it was quite complex, Dr. Carson himself compared him performing the surgery to a chef making brownies from a mix. Specifically, that the surgery was not difficult for him due to his training and expertise and because he had done it many times before. This does not mean all surgery does not carry risks, of course it does. It just means that the PN surgeons know how to perform the procedure quite well so it is not difficult for them as they have done it many times. I don't think the question of the effectiveness of the surgery should be based on its complexity, but rather if it proves to provide the intended result, such as pain relief or increased function in the case of PN surgery. I also would not necessarily conclude that a complex surgery is more risky.
PN started 2004 from fall. Surgery with Filler Nov. 2006, Dr. Campbell April 2007. Pain decreased by 85% in 2008 (rectal and sitting pain resolved completely), pain returned in 12/13. Pain reduced significantly beginning around 11/23.
-
cpps-admin
- Posts: 41
- Joined: Tue Aug 05, 2014 8:29 am
Re: Publication Abstract - A Must Read!
Once again, this excellent study goes out of its way to emphasize the "great variability of pudendal nerve anatomy". As such, there is nothing routine or easily repeatable about the operation, and comparing it to "baking brownies" is not only misleadingly glib, but also shows a lack of understanding of matters medical (your anecdotes about Ben Carson's homilies notwithstanding).stephanies wrote:It just means that the PN surgeons know how to perform the procedure quite well so it is not difficult for them as they have done it many times.
And regarding Ben Carson:
Ben Carson's patients claim malpractice in star doctor's path to politics
As former neurosurgeon launches campaign for president on public persona of caring for children, multiple cases reveal private anguish and secret settlements
... a number of Carson’s former patients and their families involved in the claims offered the Guardian a conflicting account of his near-perfect medical path toward presidential politics, detailing their continued suffering from paralysis, seizure, an uncontrollable bladder and more life-altering ordeals.
I am the admin of the member forum at a chronic prostatitis (aka CPPS) website
-
stephanies
- Posts: 692
- Joined: Mon Oct 25, 2010 3:07 am
Re: Publication Abstract - A Must Read!
I disagree with the conclusions you have jumped to in order to support your agenda.
PN started 2004 from fall. Surgery with Filler Nov. 2006, Dr. Campbell April 2007. Pain decreased by 85% in 2008 (rectal and sitting pain resolved completely), pain returned in 12/13. Pain reduced significantly beginning around 11/23.
-
cpps-admin
- Posts: 41
- Joined: Tue Aug 05, 2014 8:29 am
Re: Publication Abstract - A Must Read!
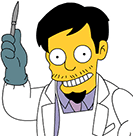
My "agenda" is to help people. I'll support anything that works, including surgery on entrapped nerves, IF the nerves are actually entrapped. 
Here is a photo of how the pudendal nerve is connected ("entrapped") by connective tissue in normal people..
Here is a photo of how the pudendal nerve is connected ("entrapped") by connective tissue in normal people..
- pudendal-nerve-attached.jpg (82.05 KiB) Viewed 1805 times
I am the admin of the member forum at a chronic prostatitis (aka CPPS) website